Anatomy of the Head and Neck
A comprehensive overview of the structural components, neurovascular supply, and clinical importance of the craniofacial region.
Osteology of the Skull
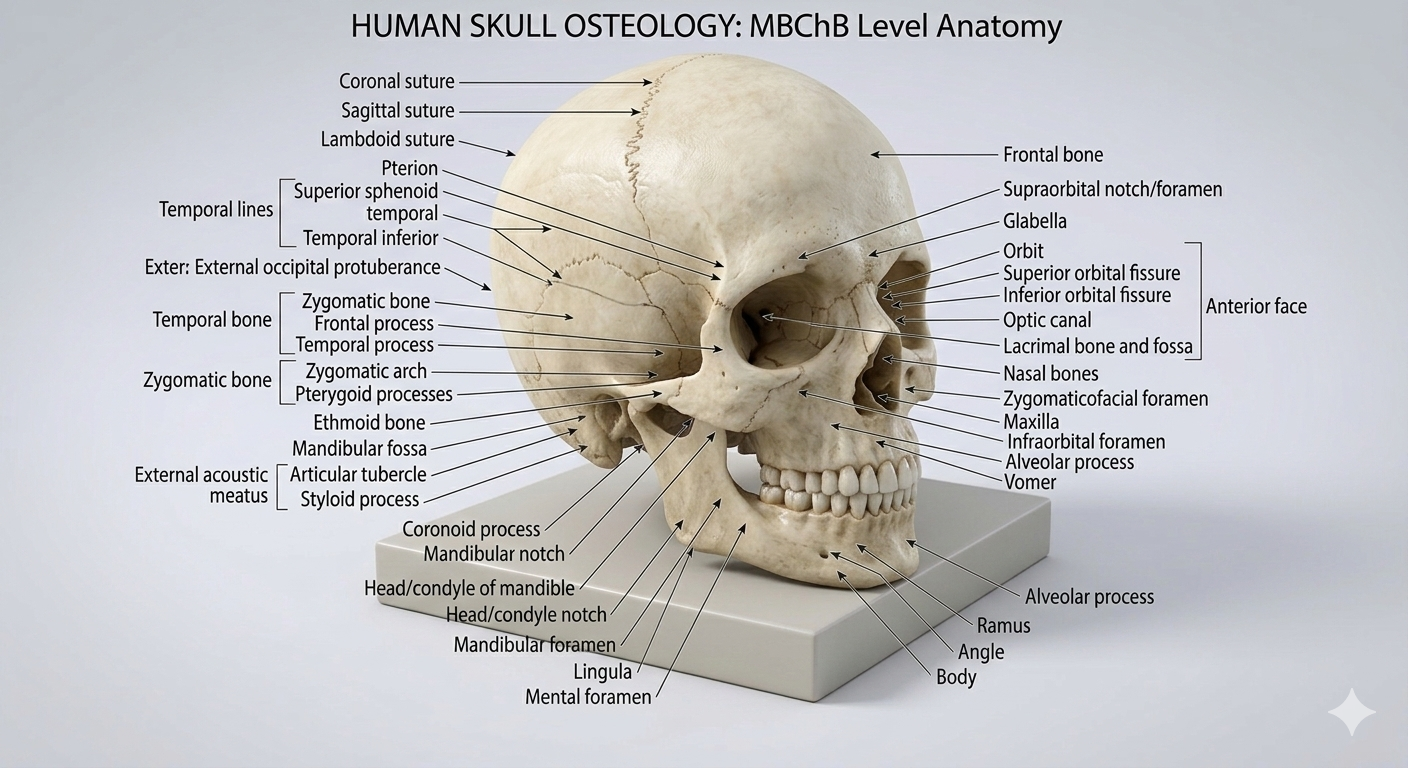
The skull is a rigid structure composed of 22 bones. It is divided into the
OSTEOLOGY OF THE SKULL – HIGH YIELD
Overview
The skull forms the bony framework of the head. It protects the brain, supports the face, and houses the organs of special senses (vision, hearing, smell, taste).
In adults, the skull consists of 22 bones joined mainly by sutures (fibrous joints).
Major Divisions of the Skull
1. Neurocranium (Cranial Skeleton)
Forms the protective case for the brain.
Bones of the neurocranium (8):
Frontal (1) – forms the forehead and roof of the orbit.
Parietal (2) – form the superior and lateral walls of the skull.
Temporal (2) – house structures of hearing and balance.
Occipital (1) – posterior skull; contains the foramen magnum.
Sphenoid (1) – central “keystone” bone of the cranial base.
Ethmoid (1) – contributes to nasal cavity and medial orbital wall.
2. Viscerocranium (Facial Skeleton)
Forms the bony framework of the face.
Bones of the viscerocranium (14):
Maxillae (2) – upper jaw, part of orbit, nose, and hard palate.
Zygomatic bones (2) – cheek bones; lateral wall of orbit.
Nasal bones (2) – bridge of the nose.
Lacrimal bones (2) – small bones forming part of medial orbit.
Palatine bones (2) – posterior portion of the hard palate.
Inferior nasal conchae (2) – increase surface area of nasal cavity.
Vomer (1) – forms inferior part of the nasal septum.
Mandible (1) – lower jaw; only movable bone of the skull.
Important Sutures
Coronal suture – between frontal and parietal bones.
Sagittal suture – between the two parietal bones.
Lambdoid suture – between parietal and occipital bones.
Squamous suture – between temporal and parietal bones.
Fontanelles (Clinical Importance)
Fontanelles are membranous gaps between skull bones in infants that allow brain growth and skull molding during birth.
Anterior fontanelle – between frontal and parietal bones; closes at ~18 months.
Posterior fontanelle – between parietal and occipital bones; closes at ~2–3 months.
Cranial Fossae (Internal Base of Skull)
Anterior cranial fossa – supports the frontal lobes.
Middle cranial fossa – contains the temporal lobes and sella turcica.
Posterior cranial fossa – contains cerebellum, pons, and medulla.
Important Skull Foramina (High Yield)
Foramen magnum – medulla, vertebral arteries, spinal root of CN XI.
Optic canal – optic nerve (CN II) and ophthalmic artery.
Superior orbital fissure – CN III, IV, V1, VI.
Foramen rotundum – maxillary nerve (V2).
Foramen ovale – mandibular nerve (V3).
Foramen spinosum – middle meningeal artery.
Jugular foramen – CN IX, X, XI and internal jugular vein.
Hypoglossal canal – hypoglossal nerve (CN XII).
Key Clinical Correlations
Temporal bone fractures may damage the middle meningeal artery, causing an epidural hematoma.
Bulging fontanelles in infants may indicate increased intracranial pressure.
Lesions at the foramen magnum may compress the brainstem and upper spinal cord.
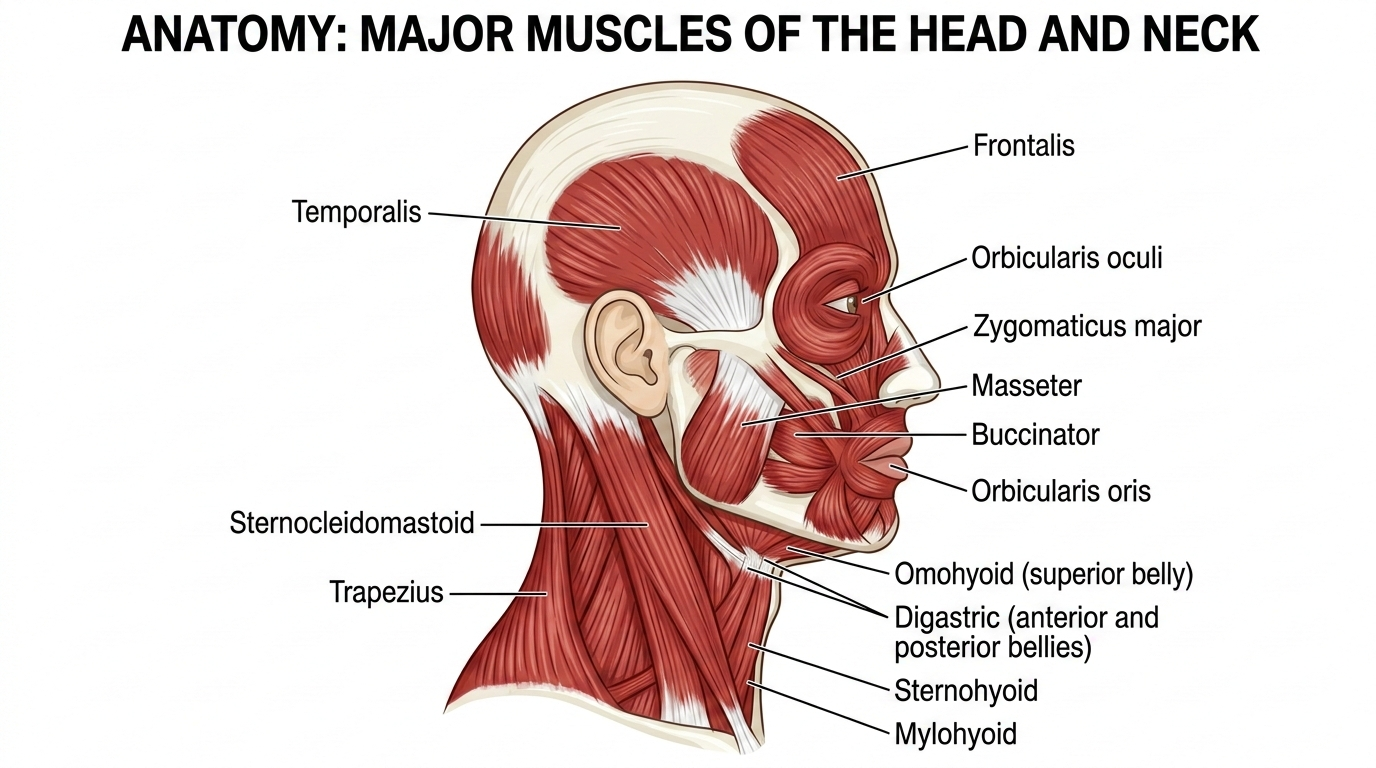
Muscles of the Head
The head contains several groups of muscles, most notably those for facial expression and mastication.
Muscles of the Head & Neck: A High-Yield Summary
This summary is organised by anatomical region and function. Focus on the origin, insertion, nerve supply (always a favourite in exams), and key action.
Muscles of the Head and Neck
1. Muscles of Facial Expression
Key Fact: These muscles are unique because they are embedded in the superficial fascia and insert into the skin. They are all developed from the 2nd Pharyngeal Arch and are therefore innervated by the Facial Nerve (CN VII).
Orbital Group
Orbicularis Oculi: Sphincter of the eyelid. Action: Closes the eye (voluntary and involuntary blinking).
Nasal Group
Procerus: Over the bridge of the nose. Action: Wrinkles the nose, draws eyebrows down (think: angry expression).
Oral Group
Orbicularis Oris: Sphincter of the mouth. Action: Closes and purses the lips (e.g., kissing, whistling).
Buccinator: Forms the muscular cheek. Action: Compresses the cheek against the teeth (helps in blowing and sucking). It is a key muscle of mastication because it holds food under the teeth.
Zygomaticus Major & Minor: Action: Draws the angle of the mouth upward and backward (smiling).
Platysma: Broad sheet in the neck. Action: Tenses the skin of the neck and draws down the lower lip (sadness/expressions of shock).
2. Muscles of Mastication
Key Fact: These act on the Temporomandibular Joint (TMJ). They are all derived from the 1st Pharyngeal Arch and are innervated by the Mandibular Nerve (CN V3).
Masseter: Most powerful. Action: Elevates and protracts the mandible (closing the jaw).
Temporalis: Fan-shaped. Action: Elevates and retracts the mandible.
Medial Pterygoid: Action: Elevates and protracts the mandible; assists in side-to-side movement (grinding).
Lateral Pterygoid: The key to dislocating. Action: Depresses and protracts the mandible (opens the mouth). Unilateral action deviates the jaw to the contralateral side.
3. Suprahyoid Muscles (Above the Hyoid)
Key Fact: These connect the hyoid bone to the skull. They form the floor of the mouth and elevate the hyoid/larynx during swallowing.
Digastric: Two bellies. Action: Elevates the hyoid, depresses the mandible.
Mylohyoid: Forms the muscular floor of the mouth. Action: Elevates the hyoid and floor of the mouth (first step of swallowing).
Geniohyoid: Action: Pulls the hyoid forward and upward.
Stylohyoid: Action: Elevates and retracts the hyoid.
Innervation Note: Mylohyoid (CN V3), Digastric (Anterior belly: CN V3; Posterior belly: CN VII), Stylohyoid (CN VII), Geniohyoid (C1 via Hypoglossal).
4. Infrahyoid Muscles (Below the Hyoid)
Key Fact: These are also called "Strap Muscles." They depress the hyoid and larynx after swallowing and during speaking.
Sternohyoid: Depresses the hyoid after elevation.
Omohyoid: Two bellies. Depresses and fixes the hyoid.
Sternothyroid: Depresses the larynx (pulls it down).
Thyrohyoid: Depresses the hyoid OR elevates the larynx (depending on which bone is fixed).
Innervation Note: All are innervated by the Ansa Cervicalis (C1-C3), except Thyrohyoid, which gets fibres from C1 via the Hypoglossal nerve.
5. Muscles of the Pharynx
Constrictors (Superior, Middle, Inferior)
Action: Constrict the pharynx sequentially to propel a bolus of food downwards (peristalsis).
Innervation: Pharyngeal plexus (CN IX & X).
Clinical Pearl: Between the base of the skull and the Superior Constrictor is a gap called the Killian's dehiscence, a potential site for a pharyngeal pouch (Zenker's diverticulum).
Longitudinal Muscles (Stylopharyngeus, Salpingopharyngeus, Palatopharyngeus)
Action: Elevate the larynx and pharynx and shorten the pharynx during swallowing.
6. Triangles of the Neck (Muscular Content)
Understanding muscle location within triangles is high-yield.
Anterior Triangle:
- Submental Triangle: Mylohyoid (floor).
- Digastric (Submandibular) Triangle: Digastric (borders), Mylohyoid (floor).
- Carotid Triangle: Contains the carotid sheath, but muscular borders are Omohyoid, Sternocleidomastoid, and Digastric.
- Muscular Triangle: Infrahyoid muscles.
Posterior Triangle:
- Occipital Triangle: Floor is made of Splenius Capitis, Levator Scapulae, and Scalenes.
- Supraclavicular Triangle: Contains the anterior scalene muscle (a key landmark for the brachial plexus and subclavian artery).
7. Prevertebral Muscles (Deep Neck)
Scalenes (Anterior, Middle, Posterior): Action: Elevate the 1st and 2nd ribs (accessory muscles of inspiration) and flex/rotate the neck. Relation: The brachial plexus and subclavian artery pass between the Anterior and Middle scalenes.
Longus Colli & Capitis: Action: Flexion of the neck and head.
8. Quick Exam Cheat Sheet
CN VII (Facial Nerve) Damage (Bell's Palsy): Loss of muscles of facial expression -> Drooping of mouth, inability to close eye (lagophthalmos), loss of nasolabial fold.
CN V3 (Mandibular Nerve) Damage: Weakness in mastication -> Jaw deviates toward the side of the lesion when opening (due to unopposed action of the Lateral Pterygoid on the healthy side).
Torticollis (Wry Neck): Tightness or spasm of the Sternocleidomastoid (SCM). Innervated by CN XI (Spinal Accessory).
Whiplash: Often involves injury to the Platysma and SCM due to hyperextension/flexion.
Neurovasculature
The arterial supply to the brain is derived from two primary pairs of arteries: the Internal Carotid Arteries and the Vertebral Arteries.
NEUROVASCULATURE OF THE HEAD – HIGH YIELD (MBChB HEAD & NECK ANATOMY)
Overview
The neurovasculature of the head consists of the arterial supply, venous drainage, and cranial nerve innervation of the scalp, face, and cranial cavity.
Arterial supply mainly arises from the internal carotid artery and the external carotid artery.
Venous drainage occurs through the facial veins and dural venous sinuses.
Neural supply is mainly through the cranial nerves, especially the trigeminal nerve.
Arterial Supply of the Head
Two major arteries supply the head:
1. Internal Carotid Artery (ICA)
Supplies the brain, orbit, and forehead.
Major branches (high yield):
Ophthalmic artery – supplies the orbit, eye, and forehead.
Anterior cerebral artery – supplies medial surfaces of cerebral hemispheres.
Middle cerebral artery – supplies lateral surfaces of cerebral hemispheres.
Posterior communicating artery – connects ICA to posterior circulation.
2. External Carotid Artery (ECA)
Supplies the face, scalp, and superficial head structures.
Important branches of the ECA (very examinable):
Superior thyroid artery
Lingual artery
Facial artery
Occipital artery
Posterior auricular artery
Maxillary artery
Superficial temporal artery
Important Arteries of the Face
Facial artery – main arterial supply to the face; tortuous course across mandible.
Superficial temporal artery – supplies scalp in temporal region.
Maxillary artery – supplies deep structures of face.
Middle Meningeal Artery (Very High Yield)
Branch of the maxillary artery.
Supplies the dura mater and skull.
Fracture at the pterion may rupture this artery, causing an epidural hematoma.
Venous Drainage of the Head
Venous blood from the head drains via:
Superficial veins – drain scalp and face.
Dural venous sinuses – drain the brain.
Important Veins of the Face
Facial vein – major vein draining the face.
Retromandibular vein – formed by superficial temporal and maxillary veins.
External jugular vein – drains superficial structures of scalp.
Dural Venous Sinuses (Very High Yield)
These are endothelial-lined venous channels located between layers of dura mater.
Major sinuses include:
Superior sagittal sinus
Inferior sagittal sinus
Straight sinus
Transverse sinus
Sigmoid sinus
Cavernous sinus
All ultimately drain into the internal jugular vein.
Cavernous Sinus (Clinically Important)
Located on either side of the sella turcica.
Structures passing through or within the cavernous sinus:
Internal carotid artery
Abducens nerve (CN VI)
Structures in the lateral wall:
Oculomotor nerve (CN III)
Trochlear nerve (CN IV)
Ophthalmic division of trigeminal nerve (V1)
Maxillary division of trigeminal nerve (V2)
Danger Area of the Face
The region from the nose to the corners of the mouth.
Facial veins communicate with the cavernous sinus through the ophthalmic veins.
Infections in this area may spread intracranially causing cavernous sinus thrombosis.
Nerve Supply of the Head
Most sensory innervation of the face is provided by the trigeminal nerve (CN V).
The trigeminal nerve has three divisions:
Ophthalmic (V1) – sensory supply to forehead, scalp, upper eyelid, and nose.
Maxillary (V2) – sensory supply to midface, upper lip, maxillary teeth.
Mandibular (V3) – sensory supply to lower face and motor supply to muscles of mastication.
Motor Innervation of the Face
Facial nerve (CN VII) supplies the muscles of facial expression.
Trigeminal nerve (V3) supplies the muscles of mastication.
Key Clinical Correlations
Rupture of the middle meningeal artery can cause epidural hematoma following temporal bone fracture.
Infections of the facial “danger triangle” may spread to the cavernous sinus.
Trigeminal nerve lesions cause loss of facial sensation and impaired chewing.
Facial nerve lesions cause paralysis of facial expression muscles.
The Circle of Willis
The Circle of Willis (circulus arteriosus cerebri) is a ring-like arterial anastomosis located at the base of the brain, specifically within the interpeduncular cistern of the subarachnoid space.
Components of the Circle of Willis
Overview
The Circle of Willis is an arterial anastomotic ring located at the base of the brain that connects the internal carotid circulation with the vertebrobasilar circulation.
It provides collateral blood flow to maintain cerebral perfusion if one major artery becomes obstructed.
Core Anatomical Components (The Arterial Ring)
The Circle of Willis is formed by the following arteries:
Anterior Components
● Left Anterior Cerebral Artery (ACA)
● Right Anterior Cerebral Artery (ACA)
● Anterior Communicating Artery (ACom)
→ Connects the left and right ACAs
Lateral Components
● Left Internal Carotid Artery (ICA)
● Right Internal Carotid Artery (ICA)
Posterior Components
● Left Posterior Communicating Artery (PCom)
● Right Posterior Communicating Artery (PCom)
● Left Posterior Cerebral Artery (PCA)
● Right Posterior Cerebral Artery (PCA)
mportant Exam Point
The Middle Cerebral Artery (MCA) arises from the internal carotid artery but does NOT form part of the Circle of Willis.
Summary of the Arterial Ring
The complete arterial circle consists of:
● 2 × Anterior Cerebral Arteries
● 1 × Anterior Communicating Artery
● 2 × Internal Carotid Arteries
● 2 × Posterior Communicating Arteries
● 2 × Posterior Cerebral Arteries
Mnemonic (Helpful for Exams)
"A A A – I I – P P – P P"
ACA – ACA – ACom
ICA – ICA
PCom – PCom
PCA – PCA
ANTERIOR CEREBRAL ARTERIES (ACA)
Overview:
The Anterior Cerebral Arteries (ACA) are paired arteries arising from the internal carotid arteries (ICA) and form the anterior portion of the Circle of Willis. They supply the medial portions of the cerebral hemispheres and play a crucial role in motor and sensory function of the lower limbs.
Origin:
● Left and right ACA arise from the terminal branches of the internal carotid arteries.
Course:
● Travel anteriorly, medially, and superiorly, passing above the optic chiasm.
● Joined across the midline by the Anterior Communicating Artery (ACom).
Branches:
● Orbital branches – supply orbital surface of frontal lobe.
● Frontopolar branches – supply anterior frontal pole.
● Medial striate arteries (recurrent artery of Heubner) – supply caudate nucleus, anterior limb of internal capsule.
● Callosomarginal artery – supplies cingulate gyrus and paracentral lobule.
● Pericallosal artery – continues along the corpus callosum supplying medial hemispheric surfaces.
Supply Territory:
● Medial frontal lobe
● Medial parietal lobe
● Superior frontal gyrus
● Paracentral lobule (motor & sensory cortex for lower limb)
● Anterior corpus callosum
Clinical Correlations:
● ACA stroke: Contralateral weakness and sensory loss in the lower limb > upper limb.
● Behavioral and personality changes due to frontal lobe involvement.
● Urinary incontinence if paracentral lobule is affected.
ANTERIOR COMMUNICATING ARTERY (ACom)
Overview:
The Anterior Communicating Artery (ACom) is a short, midline vessel connecting the left and right Anterior Cerebral Arteries (ACA), forming the anterior part of the Circle of Willis.
It provides a pathway for collateral blood flow between the hemispheres.
Origin & Course:
● Connects the distal ends of the left and right ACA.
● Lies anterior to the optic chiasm and lamina terminalis.
Branches:
● Small perforating branches to:
• Hypothalamus
• Anterior perforated substance
• Septal nuclei
Supply Territory:
● Hypothalamic region
● Parts of the basal forebrain
● Anterior septal area
Clinical Correlations:
● Most common site of berry (saccular) aneurysms in the brain.
● Rupture → subarachnoid hemorrhage (SAH).
● May cause visual field defects if compressing the optic chiasm.
● Can compromise anterior circulation collateral flow if occluded.
POSTERIOR CEREBRAL ARTERIES (PCA) – HIGH YIELD
Overview:
The Posterior Cerebral Arteries (PCA) are paired arteries arising from the terminal bifurcation of the basilar artery. They form the posterior portion of the Circle of Willis and supply the occipital lobes, inferior temporal lobes, and parts of the midbrain and thalamus.
Origin & Course:
● Arise from the basilar artery at its bifurcation.
● Course laterally and posteriorly around the midbrain.
● Connected to the internal carotid artery via the Posterior Communicating Artery (PCom).
Major Branches:
● Posteromedial choroidal arteries – supply thalamus and choroid plexus.
● Calcarine artery – supplies primary visual cortex.
● Parieto-occipital branches – supply medial occipital and parietal lobes.
● Temporal branches – supply inferior temporal lobe.
Supply Territory:
● Occipital lobe – visual cortex (primary & associative areas)
● Inferior temporal lobe
● Posterior corpus callosum
● Thalamus (via perforating branches)
● Midbrain structures (tectum, tegmentum)
Clinical Correlations:
● PCA stroke: Contralateral homonymous hemianopia with macular sparing.
● If dominant hemisphere affected → alexia without agraphia (visual word recognition deficit).
● Thalamic infarcts → sensory deficits, thalamic pain syndrome.
● Brainstem involvement → cranial nerve deficits if perforating branches affected.
POSTERIOR COMMUNICATING ARTERIES (PCom) – HIGH YIELD
Overview:
The Posterior Communicating Arteries (PCom) are paired vessels connecting the internal carotid arteries (ICA) to the Posterior Cerebral Arteries (PCA). They form the posterior portion of the Circle of Willis and provide collateral flow between the anterior (carotid) and posterior (vertebrobasilar) circulations.
Origin & Course:
● Arise from the posterolateral aspect of the internal carotid artery.
● Travel posteriorly to join the proximal PCA.
● Pass lateral to the optic tract and medial to the temporal lobe.
Branches:
● Small perforating arteries to:
• Thalamus
• Hypothalamus
• Internal capsule
Supply Territory:
● Thalamus (via perforating branches)
● Hypothalamus
● Portions of the internal capsule and basal forebrain
Clinical Correlations:
● Common site of berry (saccular) aneurysms at the ICA–PCom junction.
● Rupture → subarachnoid hemorrhage (SAH).
● Can compress the oculomotor nerve (CN III) → ipsilateral ptosis, “down and out” eye, mydriasis.
● Variations in PCom size can influence collateral circulation in cases of ICA or PCA stenosis.
BERRY (SACCULAR) ANEURYSMS – HIGH YIELD CLINICAL RELEVANCE
Overview:
Berry aneurysms are small, saccular outpouchings of cerebral arteries, most commonly occurring at the branching points of vessels in the Circle of Willis. They are prone to rupture due to hemodynamic stress at arterial bifurcations.
Common Sites (High-Yield Exam Points):
● AnterioCommunicating Artery (ACom) – ACA junction: Most frequent site (~35-40%).
● Posterior Communicating Artery (PCom) – ICA junction: Second most common site.
● Middle Cerebral Artery (MCA) bifurcation: Another frequent site.
● Other less common sites: ICA bifurcation, basilar artery apex.
Clinical Features of Rupture:
● Sudden severe headache – “worst headache of my life” (classic SAH presentation).
● Nausea and vomiting.
● Neck stiffness (meningeal irritation).
● Loss of consciousness in severe cases.
● Focal neurological deficits depending on location and mass effect.
Specific Neurological Signs:
● PCom aneurysm: Compresses CN III → ipsilateral ptosis, “down and out” eye, mydriasis.
● ACA–ACom aneurysm: May compress optic chiasm → bitemporal hemianopia.
● MCA aneurysm: May cause motor or sensory deficits in contralateral face/upper limb.
Risk Factors:
● Hypertension
● Smoking
● Connective tissue disorders (e.g., Marfan, Ehlers-Danlos)
● Polycystic kidney disease
● Family history of cerebral aneurysms
Key Exam Points:
● Most common cause of non-traumatic subarachnoid hemorrhage (SAH).
● Frequently located at arterial bifurcations of the Circle of Willis.
● Early recognition is critical to prevent re-bleeding and neurological damage.
● Imaging: CT angiography or MR angiography detects aneurysm before rupture.
The Circle of Willis is the most common site for saccular (Berry) aneurysms, particularly at the junction of the Anterior Communicating Artery.
Clinical Summary
This article provided a snapshot of the head and neck. Mastery requires understanding the spatial relationships of these vessels and nerves.